
The retina is a thin layer of nerve cells that lines the inside of the eye. In the young eye, the vitreous is in direct contact with the retina. With aging, the vitreous slowly shrinks and these fine fibers pull on the retinal surface.
The common diseases of the retina that can be treated by medical interventions or lasers are mentioned here.

Hypertensive retinopathy is damage to the retina caused by high blood pressure.
High blood pressure causes damage to blood vessels in the eyes. Hypertensive retinopathy development depends on the duration and poor control of blood pressure. Vision is usually affected at a later stage.
If you have high blood pressure, you should get yourself a fundoscopic examination.
The retinal arteries respond to high blood pressure by narrowing. Over time, the vessels become stiff and they can push on nearby retinal veins. Damage to the blood vessels can cause them to change shape over time. They may also leak, leading to retinal bleeding and swelling of the retina. The patient can also have swelling of surrounding nerves called cotton wool spots.
If the blood pressure suddenly increases, severe leakage can occur from the retinal arteries, causing bleeding within the retina and swelling of the retina and optic disc. This is called malignant hypertension.
At the early stages of hypertensive retinopathy, no specific symptom is observed. Headaches and visual disturbances such as blurred vision can occur later
Blood pressure management is the key.
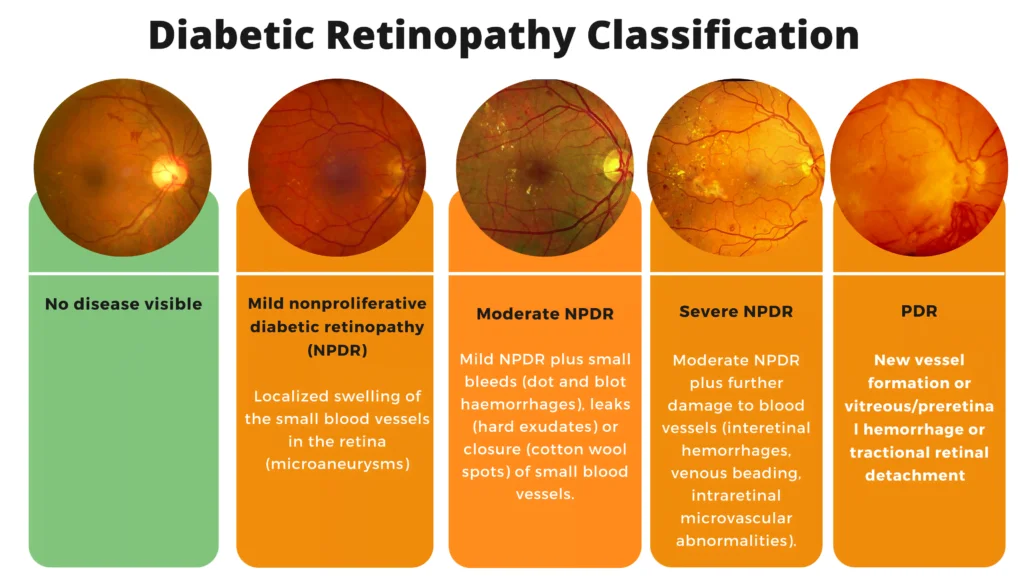
Diabetic retinopathy is one of the complications of diabetes mellitus. It affects the retina, which is the light-sensitive tissue at the back of the eye. Retinopathy occurs when diabetes damages the tiny blood vessels in the retina. This damage can lead to problems with your vision, including blindness. Diabetic retinopathy is the most common cause of blindness due to diabetes mellitus.
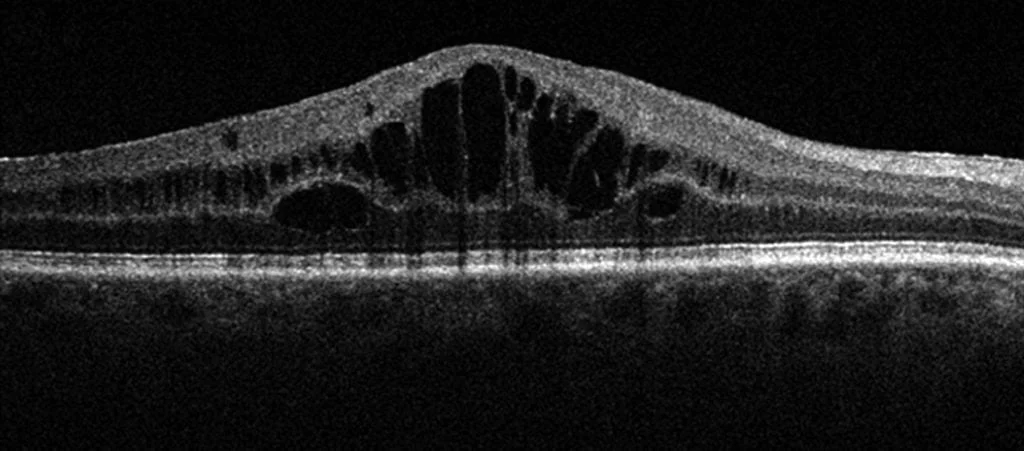
Macular edema is a painless disorder that affects the central retina or macula. When this condition is present, fluid and protein deposits collect on or under the macula of the eye.
Cystoid macular edema is a type of macular edema that includes cyst formation. The swelling may distort a person’s central vision, as the macula is near the center of the retina at the back of the eyeball.
CME is a relatively common condition and is frequently associated with various ocular conditions, such as cataract surgery, age-related macular degeneration (ARMD), uveitis, eye injury, diabetes, retinal vein occlusion, or drug toxicity. When CME develops following cataract surgery and its cause is directly related to the surgery.
Although the exact cause of macular edema is not known, it may accompany a variety of diseases such as retinal vein occlusion, uveitis, or diabetes. It most commonly occurs after cataract surgery. About 1-3 % of those who have cataract extractions will experience decreased vision due to CME during the first postoperative year, usually from two to four months after surgery. If the disorder appears in one eye, there is an increased risk of as high as 50% that it will also affect the second eye. Fortunately, however, most patients recover their vision with treatment.
Blurred or decreased central vision (the disorder does not affect peripheral or side-vision). Painless retinal inflammation or swelling. The symptoms described above may not necessarily mean that you have cystoid macular edema. However, if you experience one or more of these symptoms, contact your eye doctor for a complete exam.
It is very difficult to detect CME during a routine examination. A diagnosis is often based on the patient’s symptoms and OCT macula.
The first line of treatment for CME is usually anti-inflammatory drops. In certain cases, medication is injected near the back of the eye for a more concentrated effect. Oral medications are sometimes prescribed to reduce swelling.
Age-related macular degeneration (AMD) is a common condition affecting people age 50 years and older. This condition is associated with the loss of retinal photoreceptor cells in the center of the retina where vision is the sharpest (the macula). Macula provides the sharp vision for reading, driving and seeing fine detail. But as a rule, age-related macular degeneration does not typically lead to complete blindness.
The greatest risk factor for the development of age-related macular degeneration is age. People who are older than 50 should get regular eye exams. Having a family member with age-related macular degeneration, smoking, high blood pressure, lighter eye color, and obesity are among the risk factors for developing age-related macular degeneration. Some researchers believe that over-exposure to sunlight also may be a contributing factor in the development of macular degeneration. Women appear to be at greater risk than men. Lifestyle can play a role in reducing the risk of developing age-related macular degeneration. Eating a healthy diet high in green leafy vegetables and fish is assumed to protect against age-related macular degeneration.
When the person starts experiencing visual problems from age-related macular degeneration, symptoms can include blurred vision, blurry areas on a printed page, difficulty reading in low light levels or straight lines appearing wavy or distorted. Age-related macular degeneration reduces vision in the central part of the retina, it does not affect peripheral vision. The early stages of macular degeneration can be detected by a simple test using a chart called the Amsler grid. Waviness, distortion, or missing lines on the grid may be noticed before a change in visual acuity.
Clinically, there are two types of age-related macular degeneration ‘’dry’’ (non-neo-vascular) and ‘’wet’’ (neo-vascular) forms. Dry age-related macular degeneration is the most common form. It accounts for about 90% of age-related macular degeneration cases and is caused by the aging of the macula. Vision loss is usually gradual. Deposits under the retina called “drusen” are a common feature of dry macular degeneration. Drusen alone usually do not cause vision loss, but when they increase in size or number some people will advance to central vision loss due to geographic atrophy which is the end stage of dry form.
The “wet” form of age-related macular degeneration is a late stage of the condition and accounts for about 10% of all cases. Unfortunately, it accounts for the majority of central vision loss due to age-related macular degeneration. Vision loss may be rapid and severe. The wet type implies leakage and bleeding in the macula due to abnormal blood vessels known as choroidal neovascularization. Left untreated, these abnormal blood vessels will grow and eventually cause scarring with permanent vision loss.
To diagnose age-related macular degeneration effectively the following procedures are commonly performed: distance and near vision acuity tests, a dilated fundus examination, optical coherence tomography to obtain a clearer picture of the macula and its supporting layers, optical coherence tomography angiography and dye-assisted angiography to find abnormal blood vessels under the retina.
Currently, the only treatment for dry age-related macular degeneration is dietary vitamins and other supplements. The AREDS (Age-Related Eye Disease Study) has found that a certain combination of vitamins (vitamins C and E, lutein, zeaxanthin, and zinc) can slow the progression of dry age-related macular degeneration in people with a moderate level of disease. However, these vitamins do not cure age-related macular degeneration. The treatment of wet age-related macular degeneration has changed rapidly over the past few years. Treatment of this condition with intravitreal anti-VEGF (Vascular Endothelial Growth Factor) monotherapy is currently the standard of care. These drugs block the development of new blood vessels and limit the leakage from these vessels. They are delivered through an injection into the eye and several injections over time are usually needed. In certain types of neovascularization photodynamic therapy (PDT) can be used. Photodynamic therapy utilizes a laser beam with a light-sensitive dye to destroy unhealthy new blood vessels in or under the retina.
Visionx laser and eye clinic is comprised of the best eye doctors in Lahore. We have vast experience in diagnosing and treatment of routine and rare eye diseases. We have the best eye surgeons in Lahore and the best eye surgeons that are skilled enough for ensuring the best visual and surgical results.
A vitreous hemorrhage occurs when blood gets into the vitreous. The vitreous is a gel-like structure that fills the back of the eye. The blood blocks light rays from reaching the retina in the back of the eye. If the eye is like a camera, the retina is the thin layer of “film” that lines the back of the eye.
Signs of vitreous hemorrhage include blurred vision or seeing dark spots or floaters. Often, you may see a streak of dye rise or fall slowly, and then spread to fill the eye. If the hemorrhage is very dense, your vision may be blocked completely. In this case, you will only be able to see light and dark.
When the tiny blood vessels in the eye break, they can leak blood into the vitreous. This causes a vitreous hemorrhage. The vessels can break for several reasons:
To restore vision the blood in the cavity needs to be cleared. Your eye doctor will help you in treating this either with injections or surgery (vitrectomy) and monitor this condition until it goes away. This removes the vitreous and replaces it with a saltwater solution similar to your eye’s natural fluids. You and your doctor will discuss the course of action that is best for you.
Retinal tear and retinal detachment are part of the same spectrum of disease requiring urgent evaluation and treatment. In most cases, the patient may notice flashes and/or floaters. If the retinal tear remains unrecognized and untreated, the fluid can build up under the retina leading to retinal detachment. A retinal detachment may progress quickly and lead to complete loss of vision.
Retinal detachment most often occurs as a result of the natural aging process, but certain people are at higher risk than others. These include high myopic esp those with a history of cataract surgery, and those who have recently suffered an ocular trauma. Some types of retinal detachments can run in families.
The symptoms of vitreous separation, retinal tear, and retinal detachment are similar and sometimes can overlap. On occasion, the patient may notice floaters, flashing lights, and loss of peripheral vision which may present as a shadow moving toward the center of one’s field of vision. Floaters and flashes do not always mean that you will have a retinal detachment. But they may be a warning sign and should be evaluated promptly.
Retinal tear and retinal detachment can be recognized during dilated posterior segment examination, an examination performed on a slit lamp and magnified condensing lens.
If a retinal break can be discovered before a retinal detachment develops it can be treated with a laser to seal the break and prevent a retinal detachment. The laser creates small burns around the edges of the tear, producing scars. These scars seal the borders of the tear and prevent fluids from separating the retina from underlying tissues.
Retinal detachment almost always causes blindness unless it is treated. A detached retina is almost always repaired surgically. Surgical options include pneumatic retinopexy, scleral buckling, or vitrectomy. Pneumatic retinopexy involves injecting a gas bubble into the vitreous cavity in combination with laser surgery or cryotherapy. A scleral buckle is a tiny, flexible band that is placed around the outside of the eyeball to gently push the wall of the eye against the detached retina. Vitrectomy is the surgical extraction of the vitreous humor, reattaching of the retina, and simultaneous replacement with a dissolvable gas bubble or silicone oil.
We claim the best eye center in Lahore and one of the state of the art best eye hospital in Lahore that is equipped with the latest machinery and great ambiance. Visionx laser and eye clinic comprise all diagnostic services and you can get all eye-related services under one roof with very economical charges.
VisionX Laser and Eye Clinic are comprised of the best eye doctors in Lahore. We have vast experience in diagnosing and treatment of routine and rare eye diseases. We have the best eye surgeon in Lahore and the best eye surgeons that are skilled enough for ensuring the best visual and surgical results.
We claim the best eye center in Lahore and one of the state of the art best eye hospital in Lahore that is equipped with the latest machinery and great ambiance. VisionX Laser and Eye Clinic comprise all diagnostic services and Lasers and you can get all eye-related services under one roof at very affordable prices.
If you are near Shaukat Khanum Memorial Cancer Hospital & Research Centre or live nearby you can easily locate us by searching best eye surgeon near me or the best eye center in Lahore.